

Introduction
The spinal column, also known as the columna vertebralis or colloquially as the backbone, is the central load-bearing element in the skeletal system. It supports the body and enables an upright posture. It represents our center of rotation, making motion sequences to different directions possible. The Spine is not just the boney core, it also connects all other parts of the skeleton together. In addition, the vertebral or spinal canal encloses and protects the sensitive spinal cord that lies within it. Changes to the complex spine system may lead to impaired motion and causes severe pain. Surgical procedures on the spine are among the most frequently performed operations. A surgical procedure is often associated with pain, anxiety and limitations in your daily movements.
With our patient information we would like to tell you about different treatments for persistent symptoms in the spine.
Important information: Please keep in mind that SIGNUS Medizintechnik GmbH just provides general information about the treatment. Specific questions can only be answered by your doctor. SIGNUS assumes no liability for wrong indication or medical malpractice.

Patient information
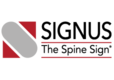
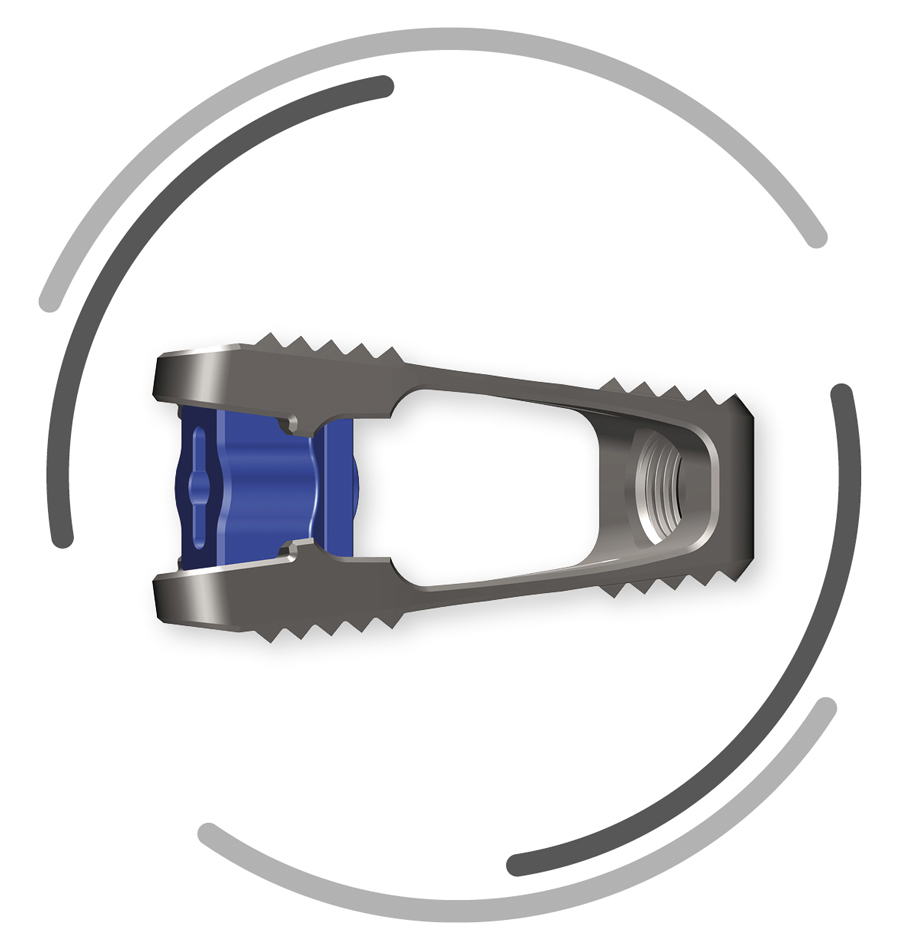
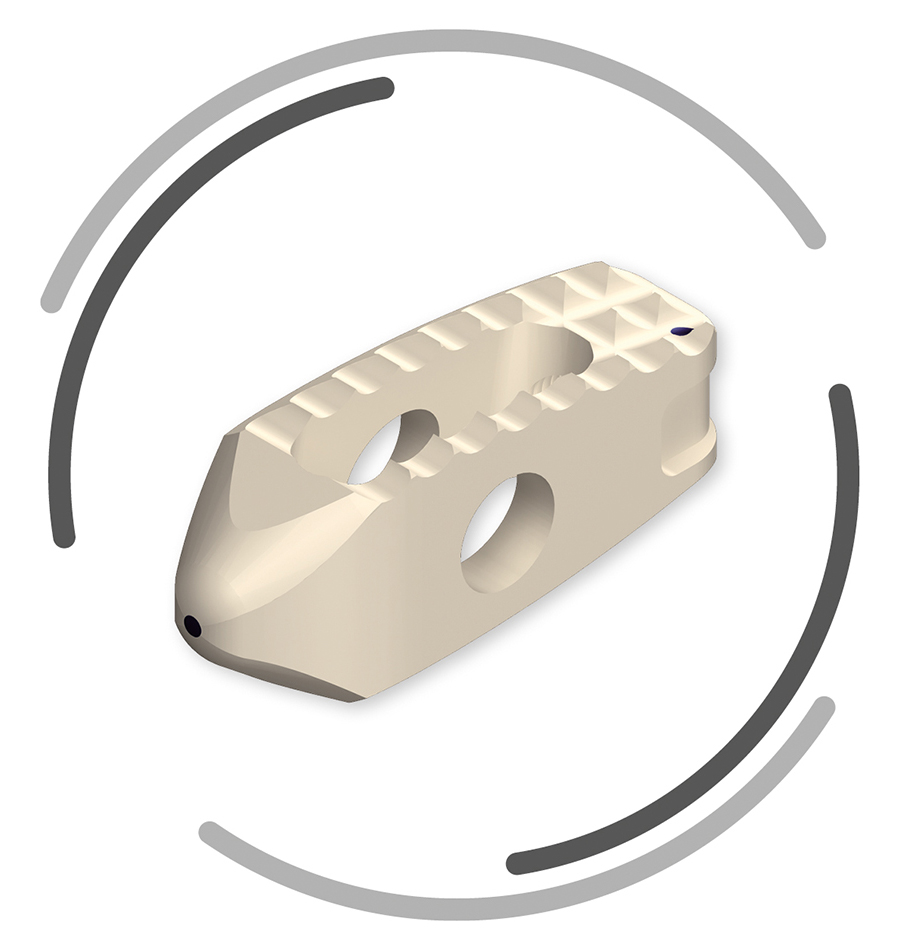
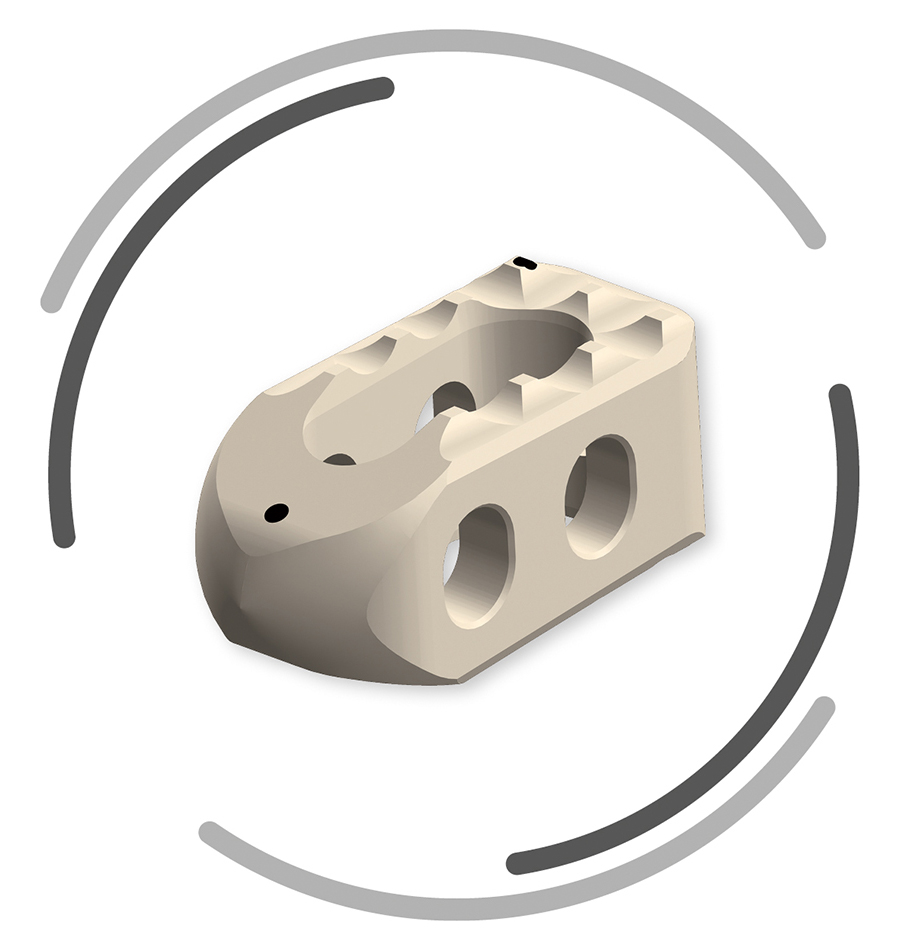
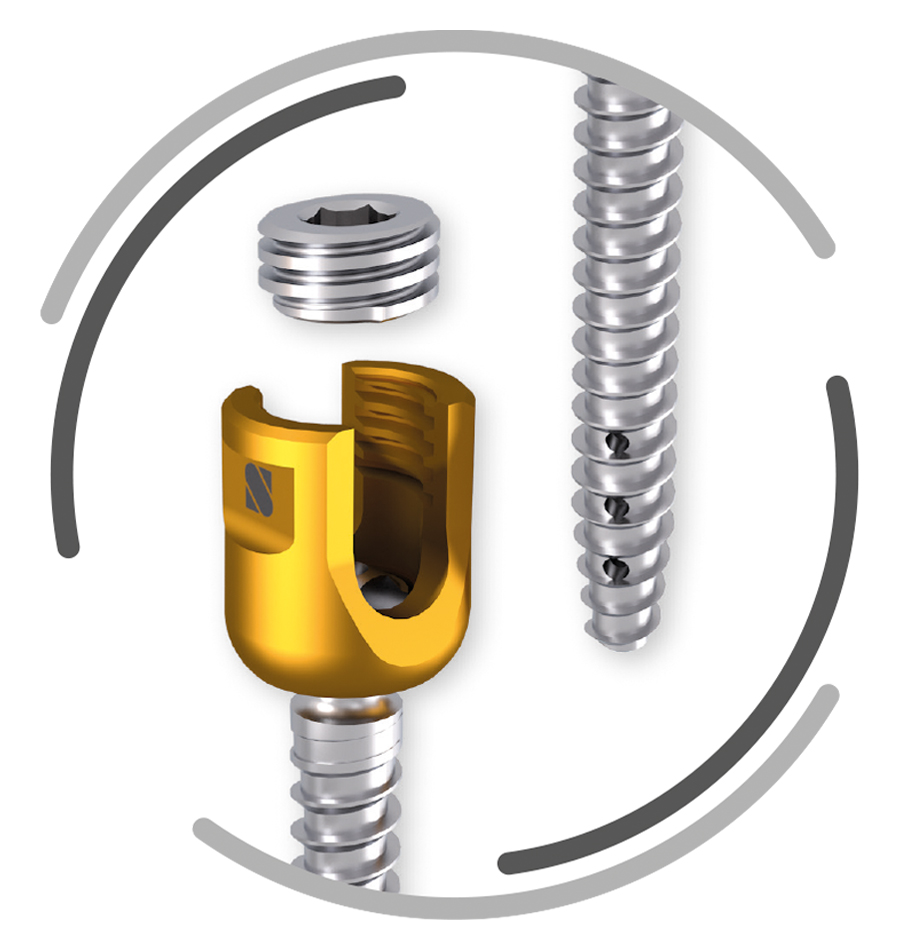
SIGNUS Products
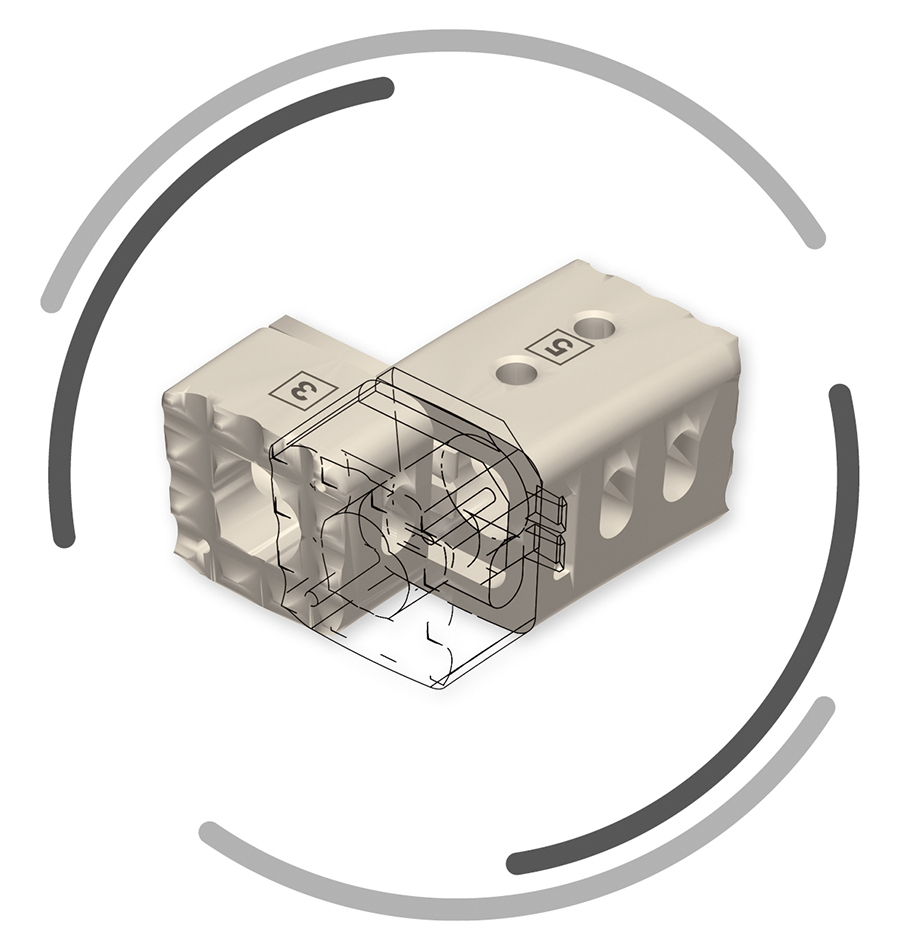
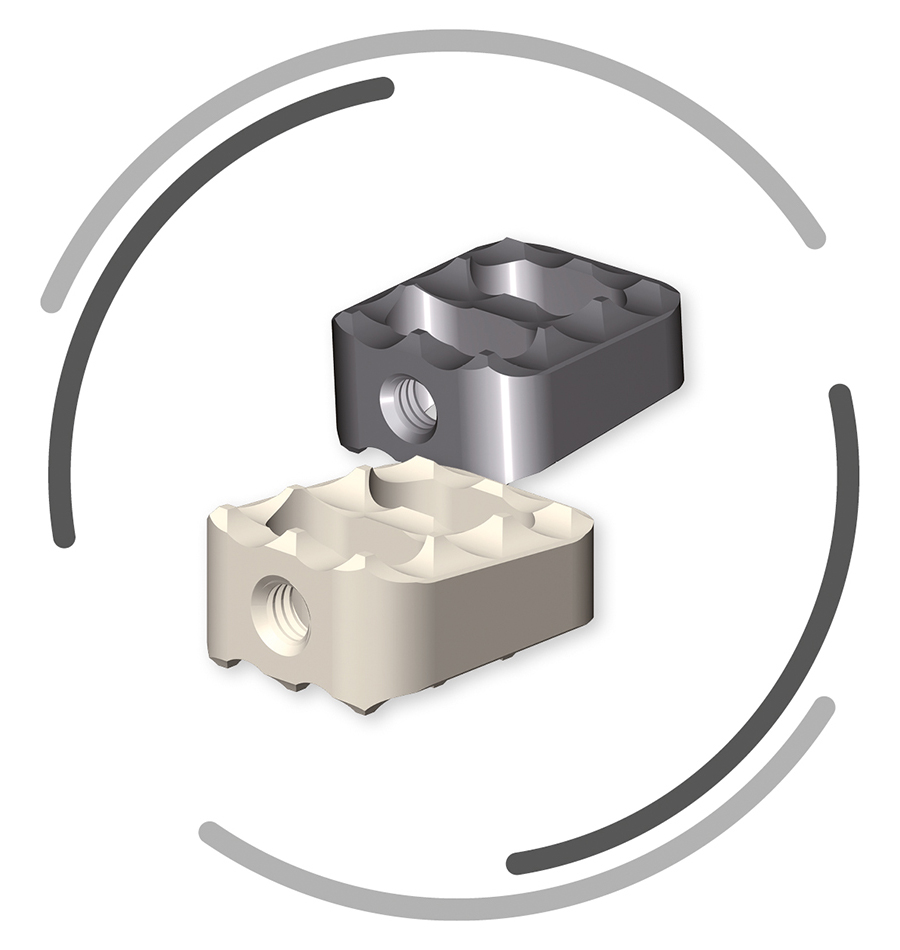
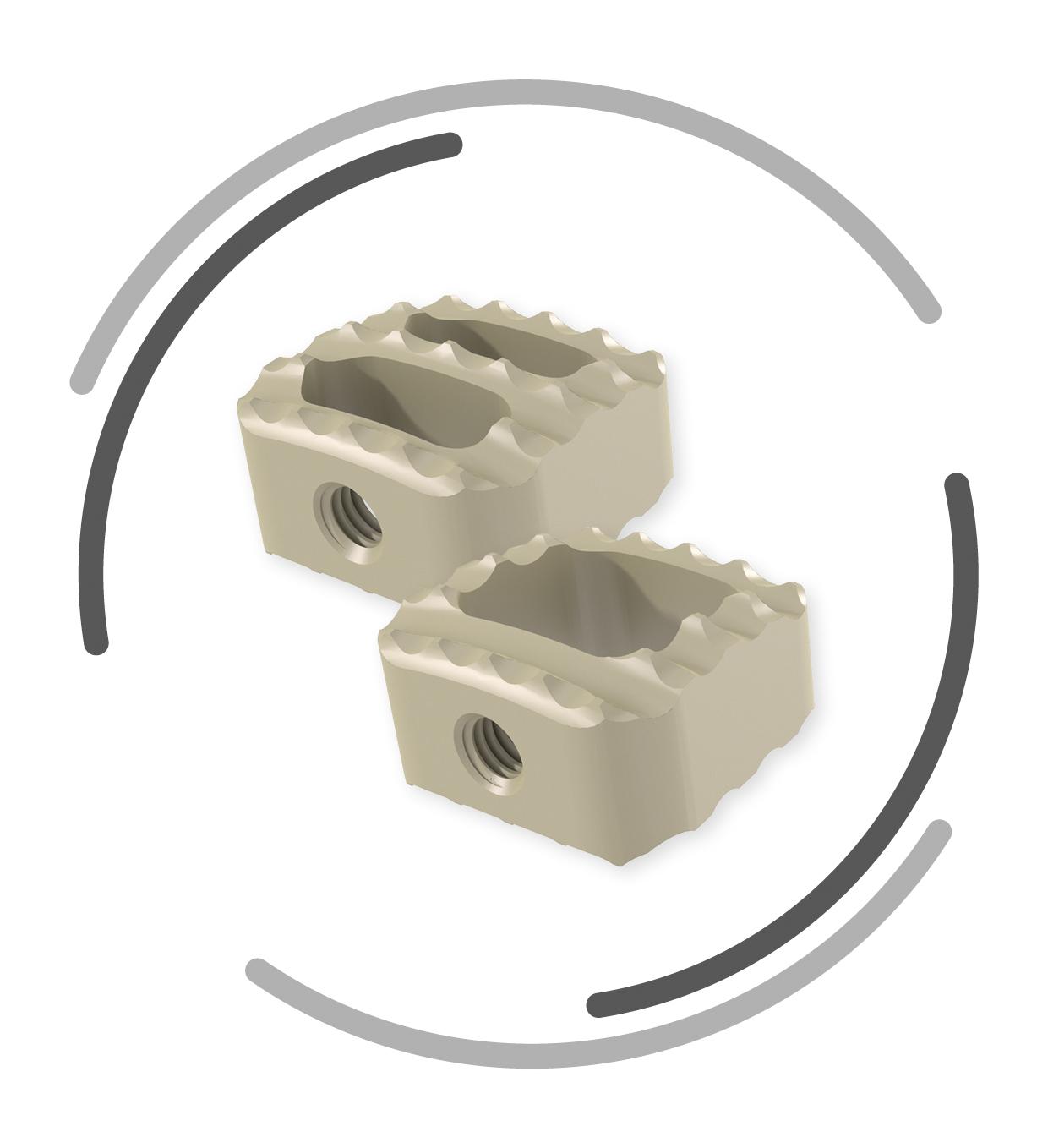
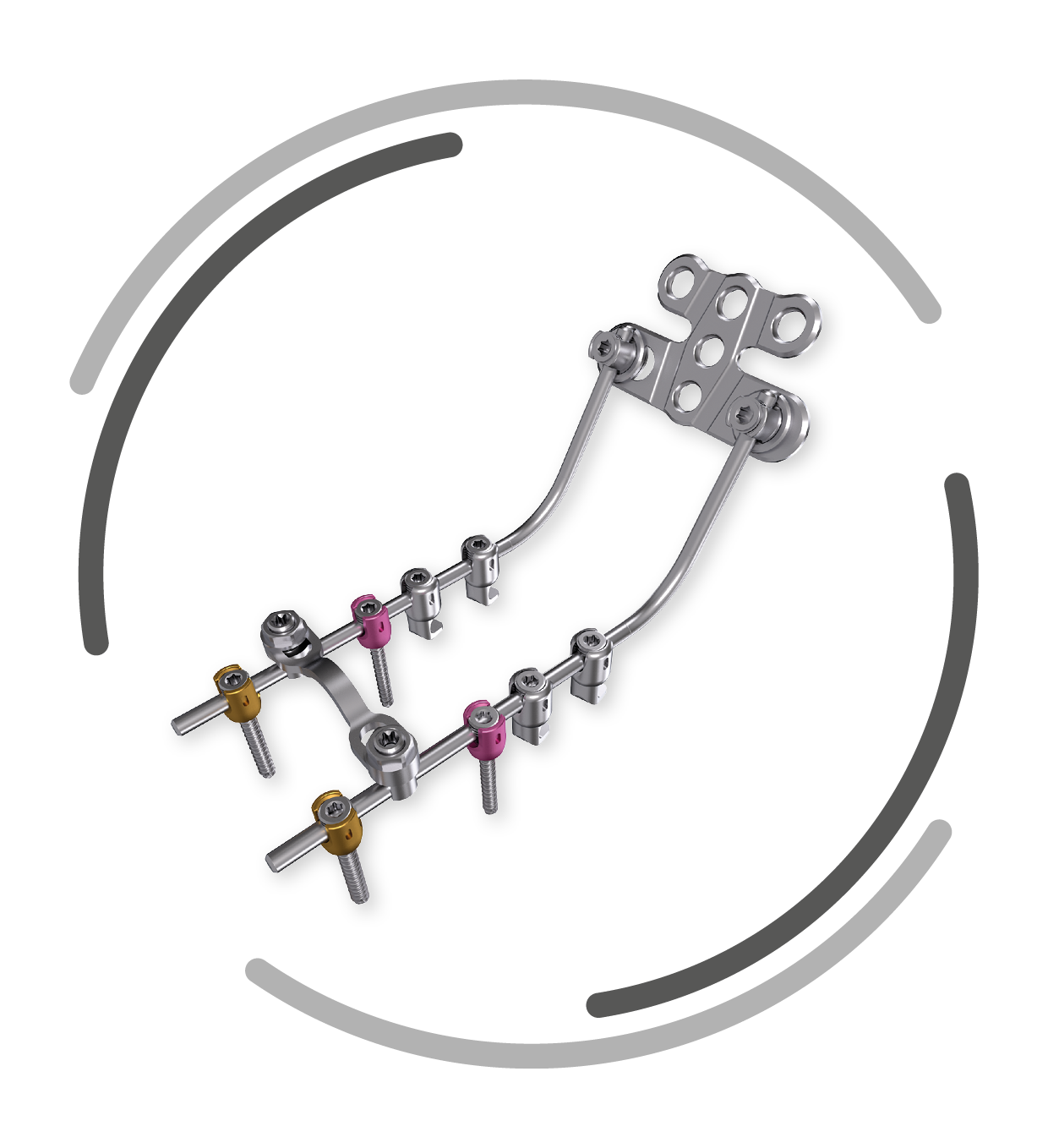
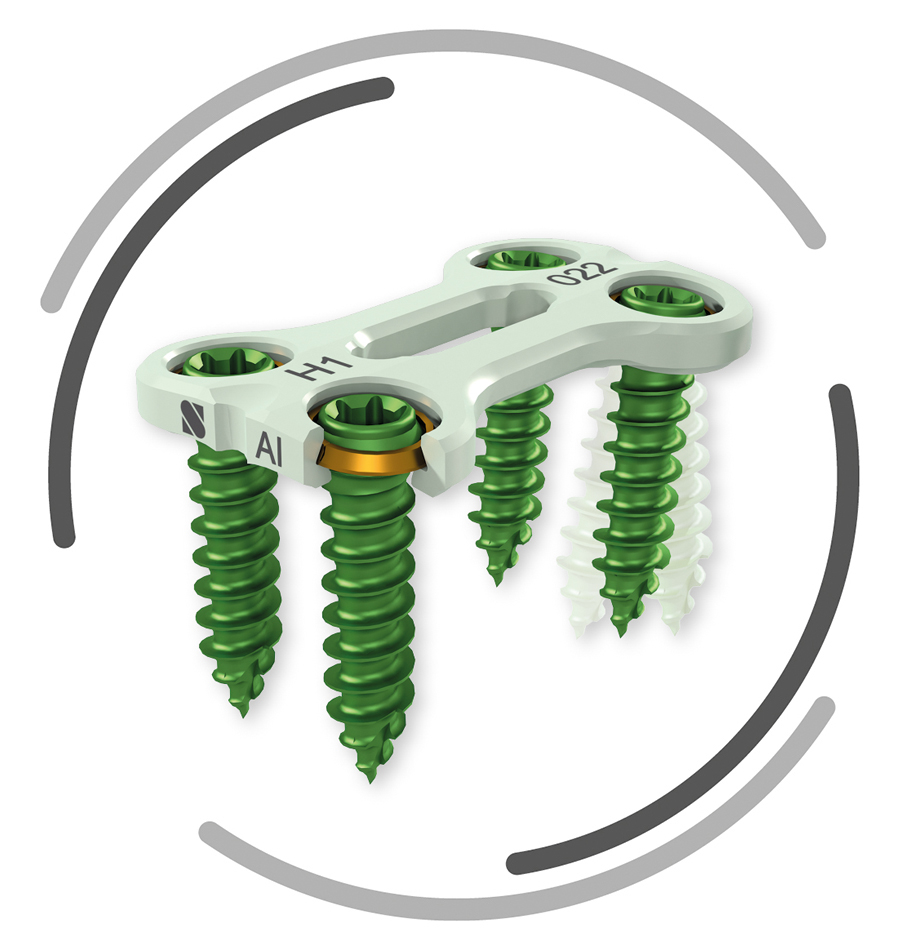

Download PDF version: VERTACONNECT






Latest News



